Endovaginal Medical Ozone Treatment as an Adjuvant in Endometriosis: A Double-Blind Randomized Controlled Trial
Jynani Pichara Morais, Carla Roberta Tim, Cintia Cristina Santi Martignago, Karina Piva Camargo Volpi, and Livia Assis
Published in Ozone: Science and Engineering, 20 March 2026. DOI: 10.1080/01919512.2026.2644229
ABSTRACT
Endometriosis is a chronic inflammatory gynecological condition that significantly impacts women’s quality of life. Given the limitations of conventional therapies, complementary strategies are being explored. This randomised, double-blind, placebo-controlled clinical trial evaluated the safety and clinical effects of endovaginal medical ozone treatment as an adjuvant intervention in women with endometriosis. Thirty participants were allocated into placebo (OzP) and active treatment (OzA) groups. Weekly endovaginal applications were performed for 10 weeks. Clinical outcomes were assessed at baseline and post-treatment using the Numeric Pain Rating Scale (NPRS), Endometriosis Health Profile-30 (EHP-30), Female Sexual Function Index (FSFI), and Beck Anxiety Inventory (BAI). The OzA group demonstrated significant reductions in pain and improvements in quality of life, sexual function, and anxiety symptoms compared with OzP. No serious adverse events were observed, and the intervention showed a favourable tolerability profile. These findings suggest that endovaginal medical ozone treatment may represent a minimally invasive adjuvant strategy in endometriosis management.
Introduction
Endometriosis is a chronic inflammatory gynecological disorder characterized by the presence of functional endometrial tissue outside the uterine cavity. Affecting approximately 10% of women of reproductive age, it is commonly associated with pelvic pain, dysmenorrhea, dyspareunia, cyclical urinary and bowel symptoms, and infertility, which may occur in up to half of patients. Although typically diagnosed in adulthood, growing evidence indicates that symptoms often begin during adolescence and are frequently underestimated in this population.
The etiopathogenesis of endometriosis is multifactorial, involving genetic, hormonal, immunological, environmental, and microbiological influences, with chronic inflammation and progesterone resistance playing central roles. Current treatments rely on medical and surgical approaches, both with relevant limitations. Hormonal therapies are often poorly tolerated, while surgery, although effective in removing lesions, is associated with symptomatic recurrence and considerable economic burden. These challenges have driven interest in noninvasive adjuvant strategies capable of modulating inflammation without the adverse effects of conventional therapies.
Medical ozone treatment has emerged as a promising integrative approach. Since its first medical applications in the 19th century, medical ozone has been shown to exert anti-inflammatory, antioxidant, regenerative, immunomodulatory, and antimicrobial actions. Its therapeutic effects are mediated by interactions with polyunsaturated fatty acids in cell membranes, generating bioactive byproducts such as ozonides and reactive oxygen species that modulate molecular and cellular pathways.
Controlled and transient oxidative stimuli induced by medical ozone are known to activate redox-sensitive signaling pathways, particularly the Keap1/Nrf2 axis. Nrf2 is widely recognised as a master regulator of cellular antioxidant and cytoprotective responses, promoting transcription of antioxidant response element (ARE)-driven genes, including heme oxygenase-1 (HO-1) and other phase II detoxifying enzymes. Nrf2 activation has also been associated with downregulation of NF-kB signaling and attenuation of chronic inflammatory responses, mechanisms directly implicated in the pathophysiology of endometriosis.
Despite its well-established role in regenerative medicine and wound care, the application of medical ozone treatment in gynecology remains underexplored. Experimental studies in animal models have demonstrated reductions in pro-inflammatory cytokines and histological improvements in endometrial tissue following local ozone application. In humans, preliminary data suggest potential benefits in endometrial receptivity and reproductive parameters, particularly when combined with pulsed electromagnetic fields. Nevertheless, the scarcity of well-designed clinical trials continues to prevent definitive validation of this therapeutic strategy.
Study Aim
Based on this background, the researchers hypothesised that local application of ozone gas may attenuate pathophysiological processes associated with endometriosis, including chronic inflammation and immune dysregulation, thereby improving clinical outcomes. The study aimed to evaluate the effects of endovaginal medical ozone treatment as an adjuvant biomedical intervention for endometriosis, contributing to the growing scientific basis for integrative and personalised therapeutic strategies.
Materials and Methods
This randomised, double-blind, placebo-controlled clinical trial was conducted at the Dr. Karina Volpe Medical and Integrative Therapy Clinic, Sao Paulo, Brazil. The study was approved by the Human Research Ethics Committee of Universidade Brasil and registered in the Brazilian Clinical Trials Registry (ReBEC, RBR-10fhfdt4).
Inclusion criteria were: women aged 20 to 50 years with a confirmed diagnosis of endometriosis (via specialised ultrasound, pelvic MRI, laparoscopy, or biopsy), presence of pelvic pain, and ability to complete questionnaires. Participants were allocated into two groups: an ozone placebo group (OzP), submitted to probe insertion without medical ozone gas, and an active medical ozone group (OzA), treated with endovaginal medical ozone. Randomisation was conducted by an independent researcher using software-generated numbers, with allocation concealed in sealed opaque envelopes. Both participants and evaluators were blinded to group assignment.
Participants underwent 10 weekly sessions over 10 weeks. Clinical outcomes were assessed at baseline and post-treatment using the following validated instruments: the Numerical Pain Scale (NPS), the Endometriosis Health Profile (EHP-30), the Female Sexual Quotient (FSQ), and the Beck Anxiety Inventory (BAI).
Ozone Treatment Protocol
All participants underwent local hygienization prior to the insertion of a sterile, siliconized, nontoxic urethral probe inserted into the vaginal canal at a depth of approximately 10 to 15 cm. Ozone was generated using a portable medical ozone generator, delivering an O2-O3 mixture at a concentration of 30 ug/mL. A total gas volume of 1000 mL was administered per session over approximately 20 minutes, corresponding to a total ozone dose of 30 mg per session. Across the 10-week protocol, the cumulative ozone dose was 300 mg per participant, with a total cumulative exposure time of 200 minutes. In the placebo group, the probe insertion was performed identically, and the same total volume of oxygen gas was used, ensuring the study remained blinded.
Results
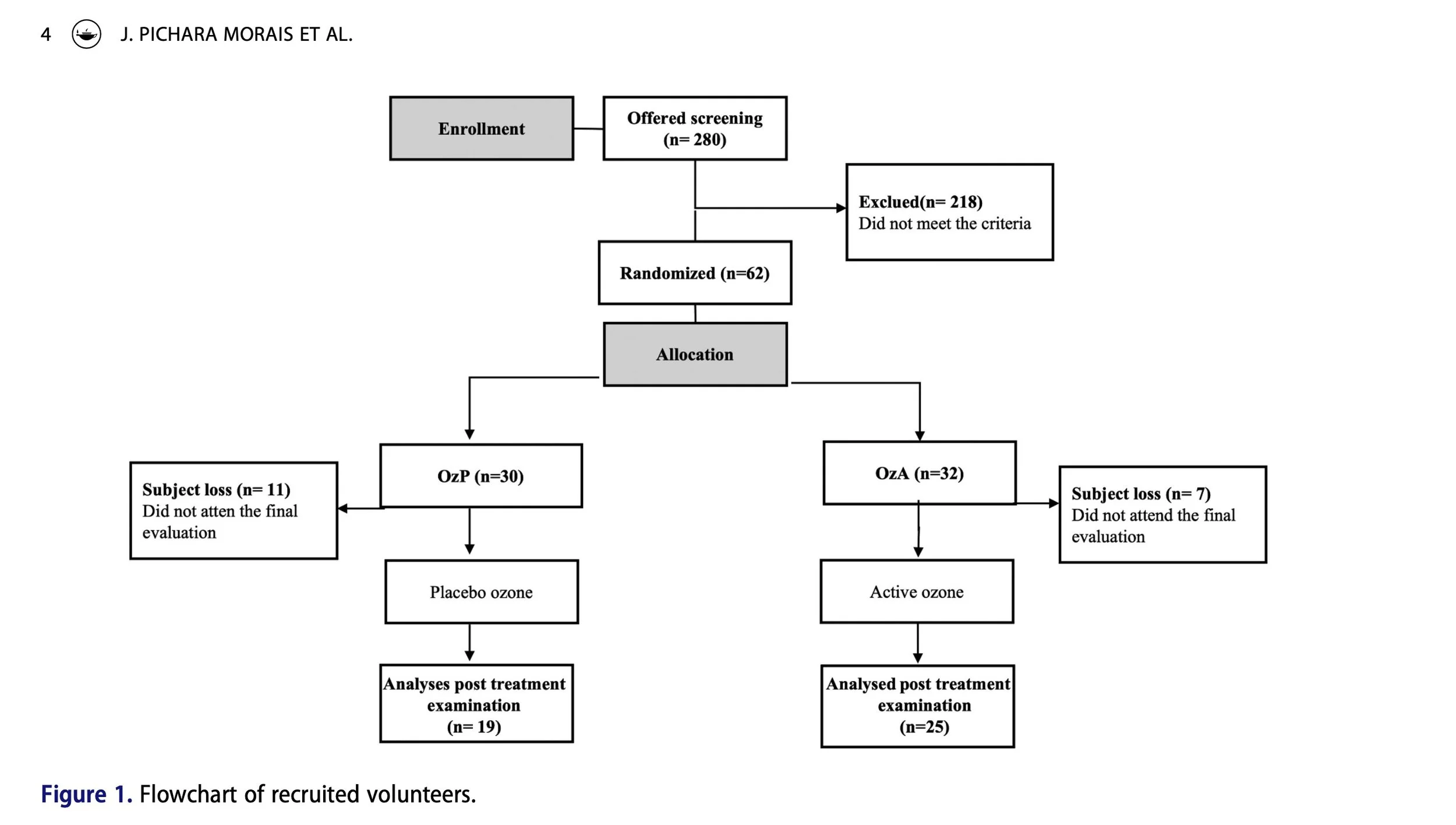
A total of 280 participants were screened; 62 met the inclusion criteria and were randomized into the two study groups. During the trial, 18 participants were excluded for missing two consecutive sessions, leaving 19 in the OzP group and 25 in the OzA group for final analysis.
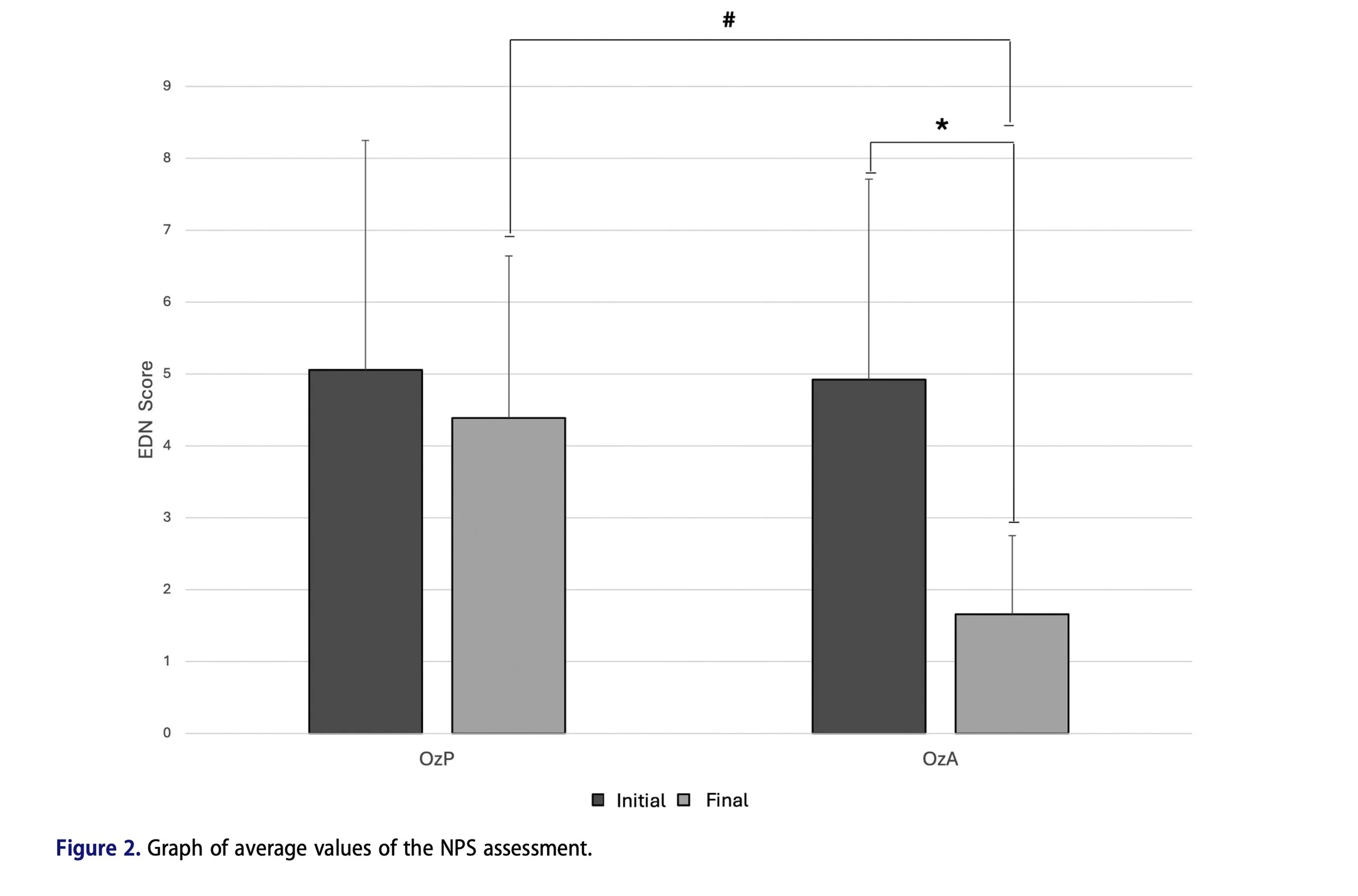
Pain (NPS): Pain scores decreased significantly in the OzA group after treatment compared to baseline (p = 0.0009). At the end of the protocol, OzA scores were also significantly lower than OzP (p = 0.0004).
Quality of Life (EHP-30): Quality of life improved in both groups, with reduced total scores in OzP (p = 0.017) and OzA (p less than 0.0001). However, OzA scores were significantly lower than OzP at the end of treatment (p = 0.0158), indicating greater improvement in the active treatment group.
Sexual Function (FSQ): Sexual function improved in the OzA group compared to baseline (p = 0.0105), though no statistically significant difference was observed between OzA and OzP at the end of treatment.
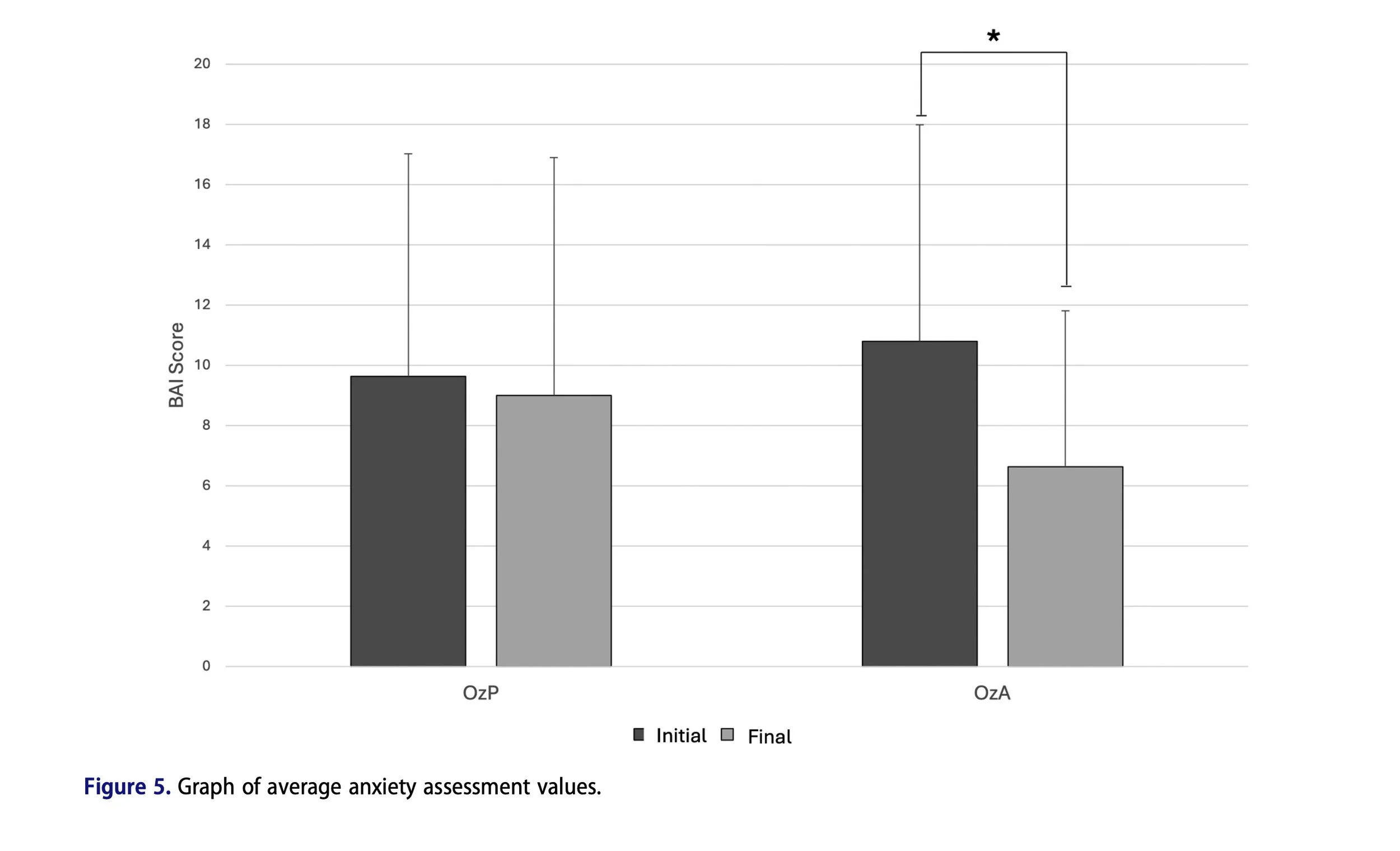
Anxiety (BAI): Anxiety scores decreased significantly in the OzA group after treatment (p = 0.0158), though no statistically significant difference was observed between groups.
Adverse Effects: Adverse effects were mild and transient, including discomfort during probe insertion in both groups and a "bubbling" sensation reported only in the OzA group. All resolved spontaneously within 10 minutes, without requiring intervention or treatment interruption.
Discussion
The study demonstrated that participants who received medical ozone treatment presented significant improvements in multiple clinical outcomes, including pain relief, improved quality of life, sexual performance, and anxiety symptoms.
The reduction in pain observed in the OzA group can be attributed, at least in part, to the neuroinflammatory modulation promoted by medical ozone treatment. Experimental studies have demonstrated that ozone application can reduce the expression of pro-inflammatory cytokines such as IL-6 and TNF-alpha, in addition to promoting histological improvement in altered endometrial tissues.
Another relevant consideration is the possible impact of endovaginal ozone application on the vaginal microbiome. Recent evidence indicates that urogenital microbiota dysbiosis may be associated with persistent inflammation and worsening symptoms in women with endometriosis. Medical ozone treatment, due to its selective antimicrobial action and immunomodulatory effect, could favour the restoration of local homeostasis, promoting a more balanced vaginal environment. The researchers note this as a biologically plausible hypothesis warranting further investigation.
At the systemic level, chronic oxidative stress plays a relevant role in the pathophysiology of endometriosis. Medical ozone treatment has been proposed as a therapeutic strategy based on its ability to induce controlled and transient oxidative stimuli capable of activating redox-sensitive adaptive pathways, particularly the Nrf2 signalling axis. Enhanced Nrf2 activity has been associated with attenuation of inflammatory signalling pathways, including modulation of NF-kB and suppression of NLRP3-mediated inflammation.

Additionally, medical ozone may directly affect nociceptive perception by stimulating the release of endogenous opioids and inhibiting pain conduction at both the central and peripheral levels. Controlled ozone application has been shown in other studies to activate endogenous analgesic pathways such as bradykinin release, modulation of prostaglandin synthesis, and increased macrophage and leukocyte activity.

All participants reported symptoms related to impaired sexual function before the start of the intervention. These findings are consistent with the literature describing pain as one of the main disruptive factors of sexuality in women with endometriosis, particularly in the form of deep dyspareunia. The improvement observed in sexual function at the end of the protocol may be associated with pain reduction and, consequently, the attenuation of psycho-emotional suffering, which reinforces the relevance of integrative therapeutic approaches in the management of endometriosis.
The proposed treatment is a minimally invasive method with simple and quick application, taking an average of 20 minutes from preparation to completion, and an affordable cost, estimated at around R$8.00 (approximately US$1.44) per session.
Limitations
The authors acknowledge several limitations inherent to the study design. The lack of longitudinal follow-up prevents definitive conclusions about the persistence of the observed therapeutic effects. Additionally, this was a single-centre study, which may limit the generalizability of the findings to other populations. Future multicenter studies involving participants with different demographic and clinical profiles, combined with biomarker evaluation, are needed to increase external validity and better elucidate the mechanistic and long-term clinical effects of this approach.
Conclusion
To the knowledge of the authors, this randomised clinical trial is among the first to evaluate the endovaginal application of medical ozone treatment in women with endometriosis. The intervention demonstrated a favourable short-term safety and tolerability profile and was associated with improvements in pelvic pain, quality of life, sexual function, and anxiety symptoms. These findings suggest that endovaginal medical ozone treatment may represent a potential minimally invasive adjuvant strategy in the clinical management of endometriosis. Further multicenter studies with larger samples, longer follow-up, and biomarker evaluation are warranted to confirm efficacy, durability of effects, and underlying mechanisms.
This work was supported by the Higher Education Personnel Improvement Coordination (CAPES). No conflicts of interest were reported by the authors.